“`html
Primobolan Tablets (Methenolone Acetate): why this “myth” still matters
Primobolan by itself is a unique anabolic steroid—and in tablet form… well… it’s definitely an exotic one. With today’s raw-material bottlenecks and extra regulations choking the UG scene, Primo sometimes feels like it’s drifting into legend.
And yet it isn’t just lore. Oral Primobolan (methenolone acetate) is still a prescription medicine in Japan. That simple fact says a lot about its footprint, tolerability, and staying power.
Quick “cred box”: still prescribed in Japan
Product: Primobolan® tablets (methenolone acetate), 5 mg.
Clinical use:
- Osteoporosis and other bone-loss states
- Severe wasting/consumption (e.g., trauma, burns, chronic illness)
- Bone-marrow failure settings such as aplastic anemia
Practical note & half-life: Labels focus on dosing and indications and don’t publish a definitive oral half-life—hence the mixed numbers you see online. Based on metabolite profiles from clinical information, I estimate ~5–10 hours. The wide range reflects limited primary data and the fact that absorption of this oral form depends mainly on gastric emptying
How to take (general info): It’s highly advised to take oral Primo with a fatty meal—it facilitates superior absorption and gives a slower, more optimal release into circulation. Some who like their orals pre-workout choose to combine it with some MCT oil; this oil can support assimilation of methenolone acetate, and MCTs are the fastest-digested fats and may be used quickly for energy—ideal as a pre-workout.
Interestingly, Primobolan Tablets are prescribed to this day under physician oversight in women, Children and, in specific circumstances, pediatrics—one reason many people consider Primo among the “safer-feeling” prescribed anabolics when kept within medical ranges. It is not the only anabolic ever prescribed for women or children (Anavar comes to mind), but it is one of the few with that history.
What makes Primo so sought-after?
Short answer: steady, believable lean-tissue progress with a side-effect profile people can live with.
Yes, Primo builds muscle. Across advanced animal work, older clinical reports, and real-world athlete experience, Primo can match testosterone’s end-point anabolic outcome—it generally takes longer to get there, but the destination can be similar.
In classic nitrogen-balance work (a distinct marker of anabolism), subjects on methenolone achieved results similar to testosterone propionate, though Primo often took longer—about 50–70% more time—to reach the same totals. Thus, in muscle-building terms Primo is slower and steadier, not flashy.
The “feel.” Compared to heavy hitters (testosterone, dianabol, deca), Primo is known for reliable, tidy progress—quality tissue instead of watery swings. People chasing a dry, athletic look tend to appreciate the difference.
Why Oral Primo is unusual (and not 17-aa)
Most oral AAS are designed to survive first-pass metabolism in the liver—why? If you swallow plain testosterone, the liver breaks it down fast before it reaches useful blood levels. That’s why orals like dianabol or anadrol use 17-alpha-alkylation (17-aa)—a chemical tweak that helps them make it through the liver, but it can increase liver strain and hurt lipids.
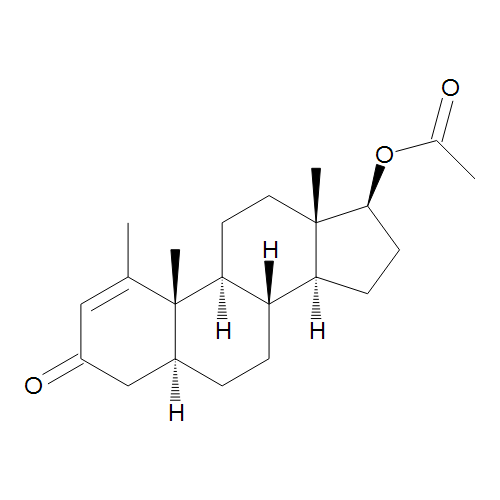
Methenolone acetate is different. It’s not 17-aa. Instead, the acetate ester increases fat-solubility and helps absorption through the gut. If you’re a bit of a chemistry geek, note that after absorption, common enzymes cleave the acetate, releasing active methenolone. The end result is an oral that delivers real systemic exposure but is generally gentler on the liver than typical 17-aa orals.
This is why I remind you again to take your Primo tabs with a small fatty snack—to support absorption—and why a few pre-workout folks use MCT oil (fast energy).
How scientists measure “anabolic” vs “androgenic”
(Skip this if you only want the bottom line, but it’s fascinating.)
When people say “Primo is more anabolic and less androgenic,” they’re leaning on bench and animal bioassays that try to separate muscle-building from masculinizing effects:
Hershberger bioassay (classic): castrated male rats receive a compound; researchers weigh the levator ani muscle (anabolic signal) and the ventral prostate/seminal vesicles (androgenic signal). The ratio between these readouts produced the folklore anabolic:androgenic numbers. Testosterone anchors at ~1:1 by convention; Primo is often reported as strongly anabolic-leaning in several setups.
Cell culture assays: muscle cells (e.g., C2C12 myotubes) and prostate cell lines are exposed to the steroid. Labs read androgen-receptor activity, protein-synthesis markers, and hypertrophy signals. These models frequently show robust anabolic signaling with methenolone and muted androgenic readouts in prostate-leaning systems compared to testosterone.
Why the lab ≠ the gym: species, dosing, route, metabolism, and tissue-specific cofactors all change the outcome. In the lab, Primo can look more anabolic than testosterone on a per-signal basis, but in real life testosterone adds mass faster because it also impacts other hormones and wider systems (e.g., water, appetite, IGF-1 dynamics). So treat the numbers as directional rather than exact. The useful takeaway is still true: Primo trends “muscle-forward, sides-back.”
You’ll also see a sky-high anabolic:androgenic ratio quoted for Primo—people toss around ~1:30 (vs testosterone’s 1:1). And you’ll hear that, in vitro, Primo can look several-fold more “anabolic” on muscle cells than testosterone while showing far less androgenic push on prostate lines. The spirit of those claims is what matters: Primo tends to favor muscle over classical androgenic baggage, even if the exact figures depend on the assay.
Why Primo shines for cutting and recomposition
Primobolan is a dehydrotestosterone (DHT) derivative. DHT is the most potent naturally occurring androgen in the body; it’s more than 3× as potent as testosterone, and it can’t convert to estrogen—the female hormone. That matters for three simple reasons:
- No aromatization. Primo doesn’t convert to estrogen, so you avoid estrogen-driven water retention and gynecomastia risk from the compound itself. That’s a huge win for the dry, carved look.
- The DHT-line “look.” DHT-family agents are associated with a tighter, leaner appearance, better nutrient partitioning, and a don’t-kill-your-appetite feel—ideal when you’re deep in a cut. Fat tissue contains plenty of androgen receptors, and Primo, like its “father,” binds them vividly, increasing fatty-acid release to the serum (= fat “incineration”). DHT also affects hormones like leptin, which can influence systemic metabolism as well as food consumption and appetite.
- Power-to-weight practicality. If your sport rewards ratio, not bulk (track, combat, gymnastics), then quality lean mass without excess water matters. Primo checks those boxes—stamina stays usable, weight stays sensible, hardness improves.
Secret-sauce detail: Plain DHT, even though it’s potent, gets rapidly inactivated in skeletal muscle by 3α-hydroxysteroid dehydrogenase (3α-HSD). Primo’s structure (a DHT derivative with a 1-methylene tweak) helps it resist that quick inactivation, so it stays meaningfully active in muscle.
Plain English: DHT burns bright but brief in muscle; Primo sticks around to do the work.
Bottom line, empirically: Primo works. It’s gentler and less dramatic than the heavy androgens (testosterone, anadrol, tren), but it trades fireworks for quality. If you’re consistent (and realistic—Primo isn’t cheap), it earns the hype.
Side effects & suppression (keep it real)
“Mild” doesn’t mean “side-effect-free.” All androgens can suppress your own testosterone production—in fancier words, they affect the HPT axis—so LH/FSH and endogenous testosterone can fall during exposure. Recovery depends on dose, duration, and what else is in the mix.
Androgenic effects—oily skin, acne, scalp shedding in those who are prone; prostate considerations in men; virilization risks in women—remain possible, especially as doses creep from medical ranges toward “performance.” Primo’s “gentle” reputation comes from its non-aromatizing DHT lineage and non-17-aa oral format—not from magic. You’re still dealing with an androgen. Respect it.
“But oral? Isn’t that liver-harsh?”
This is where Primo tablets stand out. Most orals are 17-aa to survive first pass—and that tweak is exactly why they can be rougher on the liver and harsher on lipids.
Methenolone acetate isn’t 17-aa. The acetate ester aids absorption; the body clips the ester post-absorption to free methenolone. In community terms, oral Primo is “practically gentle” compared with many orals—it has barely any impact on liver enzymes, and is seen by many as quite safe for longer-run usage. But it’s not risk-free. Lipids can still be affected over time; monitoring still matters.
Half-life and practical usage — like mentioned earlier, following metabolic patterns we may confidently put it at 5–10 hours. Hence I would recommend 2–3 daily dosages, with one pre-workout.
Primo vs Anavar vs Winstrol (fast comparison, with your tweaks)
Primo (methenolone): If you’re a woman or a senior it’s probably your first pick, if you can get a real one. Besides this, it’s ideal for contest preparations, and for this it actually combines very well with both Wini and Anavar.
Anavar (oxandrolone): DHT-line and often described as well-tolerated. Known for a clean strength/hardness bump and generally appetite-friendly feel. It is 17-aa (so mind liver and lipids). Community chatter treats it as more appropriate for shorter cycles, with some synergy alongside Primo, and less overlap with Winstrol depending on the look someone wants.
Winstrol (stanozolol): The hard/dry specialist with a strength pop. Available oral or injectable; the oral is 17-aa. People flag joint comfort issues and harsher lipid shifts more often here. It’s the most “hardcore” of the three in popular reputation, yet cheaper and more prevalent in many markets. I know more than a few IFBB pros from the ’90s and early 2000s who ran exclusively oral Winstrol plus oral Primo in the last 7–10 days before a show and swore nothing beats the quality and density it brings.
Summary vibe: Primo is the clean, steady “quality-tissue” play; Anavar adds strength and polish with a friendly feel; Winstrol is the razor-edge hardness lever with a higher side-profile—especially on lipids and joints.
Oral vs injectable Primo (the practical differences)
Oral (acetate): Convenient, non-17-aa, generally gentler-feeling as an oral. Empirically, oral Primo gives an even leaner look than the injectable; I can speculate that the shorter half-life and sharper peaks contribute to lower impact on hormones such as aldosterone that may be affected by steroids—again, nothing gives the quality oral Primo brings.
in: Long-chain depot with a longer half-life and smoother levels between pins. Typically favored for longer, more economical progress when availability isn’t an issue.
Which “feels” better? Depends on goals and context. If you want tight control and zero aromatization in an oral format, tablets make sense. If you want long-arc steadiness with less frequent administration, the depot is the classic choice.
Contest/competition note: For last-couple-of-weeks phases or meet days (track/fight), many gravitate to orals for quick adjustments and a predictable “dry” look.
FAQs
Does methenolone acetate convert to estrogen?
No. Primo is DHT-derived, so no aromatization.
Why does Primo feel “gentler” than testosterone?
Two reasons: no estrogen conversion (less water, fewer estrogenic headaches) and a lab-directional profile that leans muscle-forward and less prostate-forward. It’s still an androgen and still suppressive—just a different vibe.
Is oral Primo 17-alpha-alkylated?
No. It’s an acetate-ester oral, not 17-aa. That’s why people call it “gentler” than many orals—though liver and lipid checks are still smart.
Does Primo suppress testosterone?
Like all androgens, yes—in a dose- and duration-dependent way. Recovery speed depends on the stack, length of exposure, and individual biology.
Putting it together
Primobolan tablets are that rare mix of exotic and practical. Exotic, because very few orals deliver clean, dry progress without 17-aa baggage. Practical, because the end product—lean, believable tissue with fewer estrogenic headaches—is exactly what many people want for a cut or a recomp.
If the modern market keeps nudging Primo toward myth, remember: it’s still a real-world prescription drug in Japan, used under medical supervision for serious conditions. The legend exists for a reason.
Read this part, seriously
This post is for forum discussion/education. It isn’t medical advice, and it’s not encouragement to break any laws. AAS carry real health risks (hepatic, lipid, cardiovascular, endocrine, mood, fertility). If someone is determined to go down that road anyway, the adult move is to do it medically and legally—with baseline and follow-up labs (CBC, CMP, lipids, LH/FSH/testosterone, SHBG, estradiol), a clinician who actually knows the territory, and respect for your own longevity.
“`